 From the early 1990s until his arrest in 2002, Robert William Pickton (aka Willy) murdered—to his admission—49 women who he lured from the notorious Downtown East Side of Vancouver, British Columbia, to his pig farm in suburban Port Coquitlam. Willy Pickton’s modus operandi (MO) was to handcuff and rape the women, then shoot or strangle them to death. To dispose of the bodies, he’d butcher them in the same slaughterhouse or abattoir he processed his hogs in, then he fed the severed remains to his live pigs.
From the early 1990s until his arrest in 2002, Robert William Pickton (aka Willy) murdered—to his admission—49 women who he lured from the notorious Downtown East Side of Vancouver, British Columbia, to his pig farm in suburban Port Coquitlam. Willy Pickton’s modus operandi (MO) was to handcuff and rape the women, then shoot or strangle them to death. To dispose of the bodies, he’d butcher them in the same slaughterhouse or abattoir he processed his hogs in, then he fed the severed remains to his live pigs.
The Pickton Case, as it’s well known in Canada, wasn’t just about criminal sensationalism—something as grotesque as feeding human being parts to hungry animals. It’s a sad story of wasted human lives and a misguided mess made by human investigators. Fortunately, some good came from the Pickton Case and the parallel BC Missing Women Investigation / Missing Women Commission of Inquiry. That was better communicative cooperation between police jurisdictions and more efficient file management in missing persons cases.
Before looking at the Pickton Case outcome, let’s review who Willy Pickton was, how he managed to remain criminally active so long, and how he came to now serving the rest of his life in a maximum-security penitentiary.
 Robert William Pickton was born on October 24, 1949. He’s now 72. His parents owned the Port Coquitlam pig farm and raised Willy on it, along with his brother, David, and his sister, Linda. Willy Pickton was a reserved boy who dropped out of school at fourteen and remained working the farm after his abusive parents passed on.
Robert William Pickton was born on October 24, 1949. He’s now 72. His parents owned the Port Coquitlam pig farm and raised Willy on it, along with his brother, David, and his sister, Linda. Willy Pickton was a reserved boy who dropped out of school at fourteen and remained working the farm after his abusive parents passed on.
Court records show him to be of average intelligence but with a psychological perversion shaped by “Mommy issues”. He was very attached to his mother, regardless of her neglect of him. One notable point in young Pickton’s life was a recorded incident where, as a teen, Willy Pickton bought a calf with his own money and became very enthralled with it.
One day, he returned home to find the calf missing. He asked his mother where the calf was. She told him to go look in the slaughterhouse. He did.
There was his dead, bled, gutted, and skinned pet hanging from a meat hook.
Besides operating a pork processing plant on the farm, Willy and David Pickton ran a side business called “Piggy’s Palace”. They’d registered it as a tax-free, not-for-profit service club that leased the property to community events. Under the surface, it was a free-for-all, illegal booze-can that catered to wild parties filled with underworld characters.
Piggy’s Palace was part of the allure for the Downtown East Side of Vancouver subculture. This drug and disease-infested, civic fester was riddled with addicts and unstables who congregated in a bubble of immediacy and anonymity. These people lived for the moment, not for the day, and were perfect targets for the pig-farming predator.
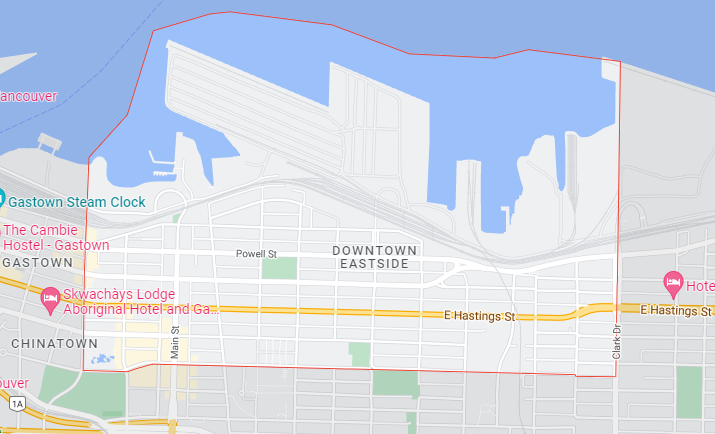
Pickton would prowl the place—generally boundaried through East Hastings with Powell Street on the north and East Pender on the south. This is right in the heart of Vancouver’s industrial waterfront. It’s only a stone’s throw from the business hub of Downtown Vancouver proper and the uber-wealth of the West End.
Willy Pickton didn’t stand out in the Downtown East Side. He fit right in. At least 49 women thought so as they accepted a ride in his beater truck back to the farm with promises of drugs and cash and fun and an escape from the streets. A permanent escape, as it happened.
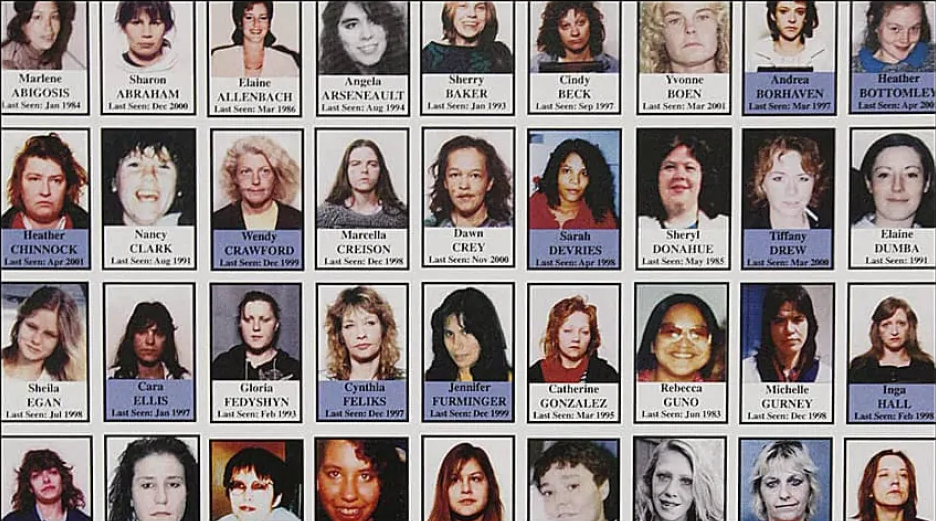
A pattern developed in the Downtown East Side. A disproportionate number of women were reported missing. They were all in similar demographics—vulnerable women who lived at-risk due to many societal issues—drug and alcohol addictions, mental illness, homelessness, victims of domestic violence, poverty, poor health, lack of education and skills, unemployable as well as being sex workers and common criminals.
The Downtown East Side law enforcement jurisdiction is owned by the Vancouver Police Department. The VPD noticed their increase in missing women reports and cautiously dealt with the matter by appointing one officer as a missing persons coordinator. Here’s where internal and external politics favored Willy Pickton.
No one in power wanted to say the “SK-Word”—Serial Killer. This would have let an uncorkable genie out of the bottle, and no one in power wanted the workload, budget drain, and social stigma/media pressure of having a serial killer running amuck in the streets of Vancouver.

So, what do good cops do in the face of bad stuff? Downplay it. Better yet, pass it off to another jurisdiction like the Coquitlam Detachment of the Royal Canadian Mounted Police—the RCMP or the Mounties.
Canadian policing structure in BC’s Lower Mainland region is rather convoluted, and this led to why Willy Pickton was hard to identify. Even harder to catch. Especially when competing jurisdictions weren’t playing for the same team.
The RCMP is Canada’s national police force They’re much like the United States FBI where they have federal responsibilities unless called or contracted by state / provincial / municipal (Muni) / civic authorities for help. Vancouver Police Department is its own LE agency, much like NYPD is or how Seattle PD operates independently of the multi-level support services like the DEA, BATF, CIA, ICE, DHLS, and a host of others.
 British Columbia’s Greater Vancouver Area (GVA or the Lower Mainland) is a hodgepodge concoction of Mountie and Muni jurisdictions. The Munis have Vancouver, West Vancouver, Delta, Abbotsford, New Westminster, and Port Moody. The Mounties have Burnaby, Surrey, Richmond, North Vancouver, Coquitlam, Langley, Maple Ridge, and Mission. Not to mention Vancouver International Airport (YVR, which is a city of its own) and another sub-city, the University of British Columbia.
British Columbia’s Greater Vancouver Area (GVA or the Lower Mainland) is a hodgepodge concoction of Mountie and Muni jurisdictions. The Munis have Vancouver, West Vancouver, Delta, Abbotsford, New Westminster, and Port Moody. The Mounties have Burnaby, Surrey, Richmond, North Vancouver, Coquitlam, Langley, Maple Ridge, and Mission. Not to mention Vancouver International Airport (YVR, which is a city of its own) and another sub-city, the University of British Columbia.
Greater Vancouver’s policing is a complex and wide-spread overlay. Vancouver’s Lower Mainland—the Fraser River Valley—population is over 3 million contained in 14,000 square miles for an average density of 214 people per square mile (PSM). That wildly ranges from 25,000 people PSM in Vancouver’s West End to practically zero on the watershed’s mountainsides.
British Columbia’s Lower Mainland has 6 municipal departments and 10 RCMP detachments. In 2002, the Munis and the Mounties had no common communication channel. Independently, they did their own thing.
The cities of Vancouver and Coquitlam-Port Coquitlam are close, distance wise. They’re 16 miles apart, as the crow flies, but Port Coquitlam is about an hour’s easterly drive in Vancouver traffic terms. Women were disappearing in Vancouver, but no bodies were being found. Vancouver women were dying in Port Coquitlam (PoCo), and their bodies weren’t being found either.
 The missing persons coordinator at VPD was vigilant in her work. She knew what was going on in the Downtown East Side. But she had no idea what was going down in PoCo. Her list—a computerized spreadsheet of missing person names, dates of disappearances, and personal items associated with each woman—was detailed and available to any LE officer with access to the Canadian Police Information Center (CPIC).
The missing persons coordinator at VPD was vigilant in her work. She knew what was going on in the Downtown East Side. But she had no idea what was going down in PoCo. Her list—a computerized spreadsheet of missing person names, dates of disappearances, and personal items associated with each woman—was detailed and available to any LE officer with access to the Canadian Police Information Center (CPIC).
The break came on February 5, 2002, when the RCMP in PoCo got informant information that something crazy was going on at the Pickton pig farm. They executed a search warrant and found items linked to several missing women the VPD coordinator listed on CPIC.
They also found human body parts including detached heads and limbs in Pickton’s freezer. In other places were severed dried skulls. They’d been Saw-zalled in half with mummified hands and feet bound inside.
The Pickton Case became a forensic first. The CSI team spent months processing dried and fresh pig manure looking for microscopic DNA profiles of Pickton’s victims. These women were:
Sereena Abotsway
Mona Lee Wilson
Andrea Joesbury
Brenda Ann Wolfe
Marnie Lee Frey
Georgina Faith Papin
Jacqueline Michelle McDonell
Dianne Rosemary Rock
Heather Kathleen Bottenly
Jennifer Lynn Furminnger
Helen May Hallmark
Patricia Rose Johnson
Heather Choinook
Tanya Holyk
Sherry Irving
Inga Monique Hall
Tiffany Drew
Sarah de Vries
Cynthia Feliks
Angela Rebecca Jardine
Diana Melnick
Debra Lynne Jones
Wendy Crawford
Kerry Koski
Andrea Fay Borthaven
Cara Louise Ellis
Mary Ann Clark
Yvonne Marie Boen
Dawn Teresa Crey
These 29 women are known Pickton victims identified through DNA. There are 13 other human female DNA profiles recovered—mired in pig shit—that haven’t been profiled to once-living women. That’s a victim count of 42. It’s 7 less than Willy Pickton confessed to killing and feeding to his pigs.
—–—
Hindsight is usually in focus. It’s been 20 years since the Pickton investigation. Learning is not just about what went wrong and improving. It’s about changing systems like communication between the Mounties and the Munis.
I was retired by the time the Pickton Case exploded. But I was a Mountie product who worked with first-rate Munis in serious crime investigations, and I have to say a murder cop is a murder cop—no matter what badge you’re wearing. We all wanted the same thing. Solve a case through admissible evidence. Bring closure to the families. And work the best we could through systematic differences.
No one in the Pickton Case investigation deliberately derailed the train. Far from it. The VPD missing persons coordinator saw the SK-Word pattern and reported it upline. Upline responded with, “Where are the bodies?” The coordinator said, “I don’t know. I just know this isn’t right and more women are going to disappear unless we dig into this.” Upline came back with, “Okay. Keep an eye, but don’t say anything to the media. We don’t need the SK-shit.”
———
 Pickton was charged with a total of 27 counts of first-degree murder. First degree, in Canada, requires the prosecution prove Pickton acted in a planned and deliberate manner on each count. If the planning point isn’t proven, but the intentional killings are still established, then the charges fall to second-degree which allows the convict an earlier parole eligibility to a mandatory life sentence, regardless of first or second.
Pickton was charged with a total of 27 counts of first-degree murder. First degree, in Canada, requires the prosecution prove Pickton acted in a planned and deliberate manner on each count. If the planning point isn’t proven, but the intentional killings are still established, then the charges fall to second-degree which allows the convict an earlier parole eligibility to a mandatory life sentence, regardless of first or second.
The trial judge severed the charges into two groups. Group A were 6 women whose evidence was materially stronger than the other 21 in Group B. The trial went ahead dealing with Group A. Group B was set aside pending the first trial’s outcome. (Note: The Group B trial never proceeded.)
A jury convicted Robert William Pickton of 6 counts of second-degree murder. How 12 jurors could think a pattern of murders was not planned but still deliberate, I can’t fathom. But whether first or second, planned or deliberate, or how many counts, is a mute legal point. Canada doesn’t have the death penalty, so Willy Pickton is going to spend the rest of his natural life in prison. There is no way this guy will ever get parole, although the law allows him to apply after 25 years of incarceration.
In the aftermath of conviction, the Pickton Case led to a lawyer-fest of appeals and inquiries. Some were cash grabs. Some were feel-goods. And some led to necessary improvements in legal and investigation procedures.
Interjurisdictional cooperation and communication were the big ones. It wasn’t just a Muni vs. Mountie thing. Munis weren’t talking to other Munis, and Mounties weren’t talking to other Mounties. In fact, the entire Vancouver Lower Mainland cop shops were acting alone. Automatously, you could say, and this was the result of years—decades—of independent police department growth in overlapping Lower Mainland communities.

Retired BC Supreme Court Justice Wallace Oppal headed the Missing Women’s Commission of Inquiry. Wally Oppal, or Stone Wally as he’s known by the police and the media, was the right man for this job. He was a highly experienced trial judge who went on to be the Attorney General of British Columbia. His 2012 report on the matter ran 1,448 pages and came back with 63 recommendations. The number 1 item, rightfully so, was amalgamating all Lower Mainland police jurisdictions—Mountie and Muni—into one regional police force.
Ten years later, this hasn’t happened. And it shows no sign of happening given the City of Surrey, the fastest growing Lower Mainland area, is forming its own police force and getting rid of the RCMP.
 However, one major intercommunication and cooperation change did occur, and it was for the better. That was forming the Integrated Homicide Investigation Team (IHIT) that makes secondments of select detectives from each department—Muni and Mountie—and has the team take over homicide cases throughout the Lower Mainland. Except for the Vancouver Police Department who still do their own thing.
However, one major intercommunication and cooperation change did occur, and it was for the better. That was forming the Integrated Homicide Investigation Team (IHIT) that makes secondments of select detectives from each department—Muni and Mountie—and has the team take over homicide cases throughout the Lower Mainland. Except for the Vancouver Police Department who still do their own thing.
The Pickton Case was a tragedy of mass proportions. It wasn’t just a fact of police failure to communicate or cooperate. It was a sad situation where a marginalized segment of vulnerable women were victimized by an unchecked demon. Here are some quotes from the Oppal report:
“The police investigation into the missing and murdered women were blatant failures.”
“The critical police failings were manifest in recurring patterns that went unchecked and uncorrected over many years.”
“The underlying causes of these failures were themselves complex and multi-faceted.”
“Those causes include discrimination, a lack of leadership, outdated police procedures and approaches, and a fragmented policing structure in the Greater Vancouver region.”
“While I condemn the police investigations, I also find society at large should bear some responsibility for the women’s tragic lives.”
“I have found that the missing and murdered women were forsaken twice. Once by society at large and again by the police.”
“This was a tragedy of epic proportions.”
 Outside of the trial and commission of inquiry, the Vancouver Police Department did an extensive internal review. Honorably, they owned the problem and vowed to change procedures in missing persons cases. Deputy Chief Doug LePard, who headed the probe, had this to say at a public news conference:
Outside of the trial and commission of inquiry, the Vancouver Police Department did an extensive internal review. Honorably, they owned the problem and vowed to change procedures in missing persons cases. Deputy Chief Doug LePard, who headed the probe, had this to say at a public news conference:
“I wish from the bottom of my heart that we would have caught him sooner. I wish that, the several agencies involved, that we could have done better in so many ways. I wish that all the mistakes that were made, we could undo. And I wish that more lives would have been saved. So, on my behalf and behalf of the Vancouver Police Department and all the men and women that worked on this investigation, I would say to the families how sorry we all are for your losses and sorry because we did not catch this monster sooner.”