 On February 26, 2025, the decomposing bodies of legendary Hollywood actor Gene Hackman and his wife Betsy Arakawa were found inside their cloistered estate at Santa Fe, New Mexico. The medical investigator ruled both died of natural causes approximately five days apart—Arakawa passing on February 12, and Hackman being deceased on February 17. There was no evidence of foul play or accident, but there is a sad and compelling story behind the tragic deaths of Gene Hackman and Betsy Arakawa.
On February 26, 2025, the decomposing bodies of legendary Hollywood actor Gene Hackman and his wife Betsy Arakawa were found inside their cloistered estate at Santa Fe, New Mexico. The medical investigator ruled both died of natural causes approximately five days apart—Arakawa passing on February 12, and Hackman being deceased on February 17. There was no evidence of foul play or accident, but there is a sad and compelling story behind the tragic deaths of Gene Hackman and Betsy Arakawa.
The bodies were discovered by maintenance workers who became suspicious as neither Arakawa nor Hackman had been seen in some time. They peered through a window and saw a body on the floor. Police immediately attended as did death scene examiners from the New Mexico Office of the Medical Investigator.
Autopsy and investigation information was released to the public on March 7. “It is unprecedented for the Office of the Medical Investigator to make public statements about sudden death investigations so soon in the process. However, the circumstances surrounding these two deaths require accurate dissemination of important information,” the New Mexico Chief Medical Investigator Dr. Heather Jarrell said at a press conference.
This was a prudent move given the high-profile nature of the Hackman-Arakawa case. In the nine days between the body discoveries and the conference, the media—especially social media—was alive with rumours and false assumptions. It’s to be expected with someone as well known as Gene Hackman and the strange circumstances of this death case.
Although the autopsy reports and scene imagery were quickly sealed by a judge acting on a petition from the Hackman-Arakawa estates, the medical investigator did offer a clear account of the death causes and the circumstances leading up to their tragic demise. Here’s what’s publicly known.
Betsy Arakawa, age 64, was last seen alive between 3:30 and 5:00 pm on February 11. She was filmed on surveillance cameras at Sprouts Farmers Market, CVS Pharmacy, and a pet food store in downtown Santa Fe. Her car entered the couple’s gated community at 5:15 pm using the remote control assigned to her. Cell phone records and inquiries established she’d called a private medical clinic on the morning of February 12 and made an afternoon appointment with a doctor. She never showed up.
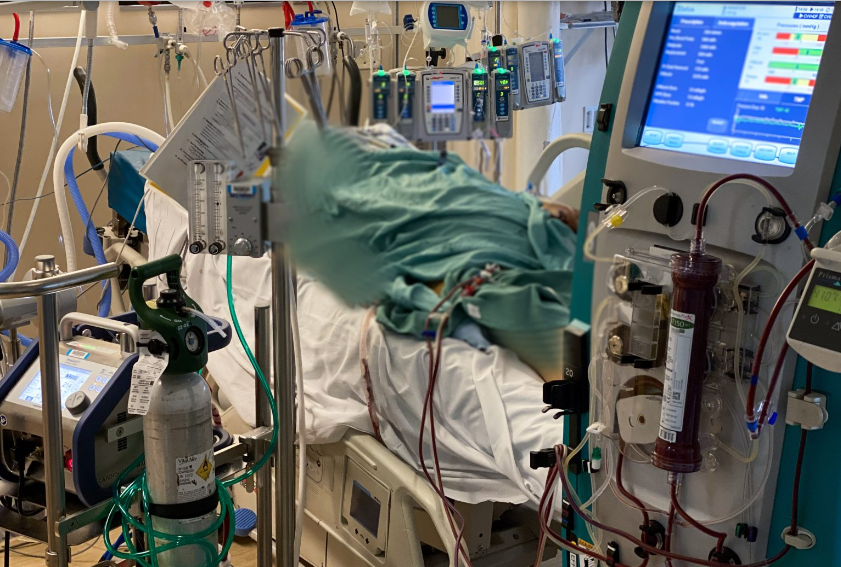
Arakawa’s body was positioned on the floor of one of their home’s bathrooms. An open vial and scattered pills were near her, but the medical examiner determined they were a routine prescription for a thyroid condition and had nothing to do with her death. It seemed she’d suddenly collapsed, became unconscious, and shortly died.
Her autopsy showed a serious lung condition, and she suffered from an escalating case of hantavirus infection. Without question, this proved fatal and Hantavirus Pulmonary Syndrome (HPS) clearly was the cause of her death. Hantavirus primarily infects rodents and is highly transferable to humans. The death scene property outbuildings showed evidence of deer mouse infestation which results in airborne particles from droppings or discharges being human-inhaled. HPS can manifest in the body for weeks before sharply increasing in respiratory difficulties and then sudden death.
Hantavirus Pulmonary Syndrome is rare, but the State of New Mexico Health Department recorded 136 infections over the last 50 years. Nearly half of the cases were fatal. HPS is treatable if caught in the early stages, but the autopsy conclusions found Betsy Arakawa was in an advanced, chronic condition. Likely, the rapidly escalating symptoms is why she made the doctor appointment and why she expired so quickly.
Gene Hackman was already aged and frail. He was 95 when he died, and his autopsy showed he was in an advanced stage of dementia—confirmed in the brain dissection and MRIs as Alzheimer’s Disease. Hackman also suffered from significant atherosclerotic cardiovascular disease (plaque-clogged heart arteries) as well as renal disease (failing kidneys).
The medical investigator ruled Gene Hackman’s cause of death was due to complications from heart failure, dementia, and his kidneys shutting down. This is also known as Multiple Organ Dysfunction Syndrome (MODS) and is a common end-of-life condition for the very elderly. Basically, the body progressively quits.
There was strong evidence for Hackman’s death date of February 17. That was the day his pacemaker stopped which is proof of death. Although there’s no doubt about where, when, and how Hackman died, the disturbing and unanswered question is what he knew—what he was aware of—while his wife—his sole caregiver and life support system—lay deceased and decomposing on the bathroom floor. This is truly tragic. Just awful to think of that helpless and alone old man.
Additionally tragic is that one of the couple’s dogs also died during the time Hackman and Arakawa went undiscovered. The animal was recovering from a veterinary procedure and was kept caged. The poor pet probably succumbed to dehydration.
In the time after the body discoveries on February 26 and the official information release on March 7, a lot of media speculation went on about the states of the Arakawa and Hackman corpses, specifically around the reports/rumors of mummification. This has been clearly addressed by forensic pathologist Dr. Judy Melinek in her article on MedPageToday.
Long-term followers of DyingWords.net may remember Judy when she guest posted on this site corresponding to the release of her first book Working Stiff: Two Years, 262 Bodies, and the Making of a Medical Examiner which documented her World Trade Center bombing experience.
Here’s Dr. Melinek’s piece titled Gene Hackman’s Death: How the Mystery Unfolded — Determining time of death can help inform the cause of death.

When actor Gene Hackman and his wife, pianist Betsy Arakawa, were found dead and decomposed in their Santa Fe, New Mexico home on February 26, much of the media fixated on a phrase in the police report describing “mummification” of their hands and feet. People who hear that phrase tend to immediately think of embalmed cadavers from ancient Egypt, as seen in bad movies.
The medical term, however, describes a natural process of postmortem change. Mummification of the extremities occurs as a process of desiccation: the skin dries out, turns brown, wrinkles up. We usually find it in a warm, dry environment, and though it can happen over the course of weeks, it might also set in as quickly as a matter of days.
Given that these two decedents were found indoors in arid Santa Fe, and that there was a space heater in the bathroom near Arakawa’s body, the finding of mummification is not surprising. Subsequent interrogation of Hackman’s pacemaker indicated that the last cardiac activity was on February 17 — 9 days before the bodies were found — and that workers had last been to the residence approximately 2 weeks prior. Meanwhile, Arakawa was last seen on the gated community CCTV and was communicating via e-mail on February 11.
It’s these circumstantial bits of information from the scene that are often the most helpful clues in narrowing down the time of death in the early phases of a death investigation. Let’s dive deeper into the role of a forensic pathologist and other key players in a mysterious case like Hackman and Arakawa’s.
Narrowing Down Time of Death
Time of death estimation is a complex process that depends on multiple factors both intrinsic to the body and found in the immediate environment around it. These variables can include the body’s weight and clothing, the ambient temperature, whether the death occurred indoors in a controlled environment or outdoors where temperatures fluctuate, the health status of the individual just prior to death, and the presence or absence of animals (including insects) that can feed on the body.
Experienced forensic pathologists carry around a mental library of cases that inform us over the course of a career of what a decomposing human body will look like after 24 hours, 48 hours, weeks, and months — and in all different ambient conditions. Death scene investigators can also take a measurement of the core body temperature at the scene that we can compare to published data to help narrow down a tighter death interval using nomograms opens in a new tab or window.
Post-mortem interval estimation isn’t perfectly empirical, but its reliability increases with each bit of information gleaned about a case, the forensic expertise of the person doing the assessment, and the thoroughness of the police investigation. It’s often our role early on to help the police focus their investigation on a reasonable time frame by providing a ballpark estimate of when the person died, and to help them dismiss incompatible testimony or unlikely suspects.
The Cause of Death
What about the cause of death? You have to be concerned about an environmental toxin like carbon monoxide or natural gas when two people and a pet are dead in the same enclosed residence. So, hazardous-materials crews would need to assess such a scene prior to arrival of medical first responders, who might otherwise be putting their own lives at risk. Environmental testing was performed at the residence of Hackman and Arakawa, and additional carbon monoxide testing was also performed on the human remains. All these tests were negative.
The deaths remained a mystery until Friday, March 7, when the medical examiner held a news conference to report that Arakawa had died from hantavirus, a rare pathogen that can be transmitted from rodent droppings, and that Hackman, who had been suffering from Alzheimer’s and cardiovascular disease and had relied on his wife’s care, likely died of heart disease opens in a new tab or window in the same house a week later. It’s not clear if Hackman knew his wife was dead.
This is a heartbreaking conclusion. It came after extraordinarily intensive and quick work by New Mexico’s state Office of the Medical Investigator (OMI) and underscores their dedication and professionalism. The New Mexico OMI has extensive experience with infectious diseases and is one of the select death-investigation facilities in the U.S. with a BSL-3 biosafety level morgue where they can handle infectious agents that spread through airborne transmission.
I suspect that there might have been signs at autopsy that pointed to a lung infection, and that hantavirus was then detected by identifying its genetic signature through polymerase chain reaction (PCR) testing of a nasopharyngeal or lung tissue swab. The Hackman-Arakawa property was in a remote area of Santa Fe, and there was evidence of rodent activity there. The couple had three dogs, and sometimes pets can come in contact with wild rodents and bring them into the house. The necropsy on the dead dog is still pending and may answer more questions about the source of viral exposure.
The Risk of Isolation
I know a lot of gut-wrenching death stories, and the worst ones always involve either the feeling that death may have been preventable, or that the decedent suffered. Everyone who’s been following this shocking and complex public mystery should be grateful to the New Mexico OMI for giving us — and the Hackman-Arakawa family — a speedy and decisive resolution.
If you have people in your lives who are the sole caregivers to a medically fragile patient, please reach out frequently to give them as much help and support as you can. Balancing their need for privacy with your own concerns for their wellbeing is never simple, but maybe these public deaths will open conversations with them about a less isolated environment for their end-of-life care.
Judy Melinek, MD, is an American forensic pathologist currently working as a contract forensic pathologist in Wellington, New Zealand. She is the co-author with her husband, writer T.J. Mitchell, of the memoir Working Stiff: Two Years, 262 Bodies, and the Making of a Medical Examiner, and the forensic-detective novels First Cut and Aftershock. You can follow her on BlueSky @drjudymelinek and Facebook/DrJudyMelinekMD.
— — —
Tragic is an appropriate word to describe the Hackman/Arakawa death case. Here was once an A-List, Oscar-winning movie star and now a very wealthy man living a recluse life with his also-accomplished wife of 30 years. They have no contact with the outside for two weeks, and no one in the family or friend sphere thinks to check on them. An old, frail, and demented man and his increasingly ill younger wife die alone, days apart, and rot on the floor of their multi million-dollar mansion.
The magazine Architectural Digest once ran a feature on the Hackman/Arakawa Santa Fe home. Here’s some pictures of it. It makes one think.