 Imagine a serial killer causing 256 deaths in your town—within the first four months of this year. Your place would panic. Your doors would be locked. Windows barred. Your streets would be bare with the cops falling flat-out to find the fiend. Does this sound like a far-fetched plot for the next best-seller? Nope. It’s real. It’s happening right here at home and the killer is known. Her name is Fentanyl. She’s heroin’s deadly little sister.
Imagine a serial killer causing 256 deaths in your town—within the first four months of this year. Your place would panic. Your doors would be locked. Windows barred. Your streets would be bare with the cops falling flat-out to find the fiend. Does this sound like a far-fetched plot for the next best-seller? Nope. It’s real. It’s happening right here at home and the killer is known. Her name is Fentanyl. She’s heroin’s deadly little sister.
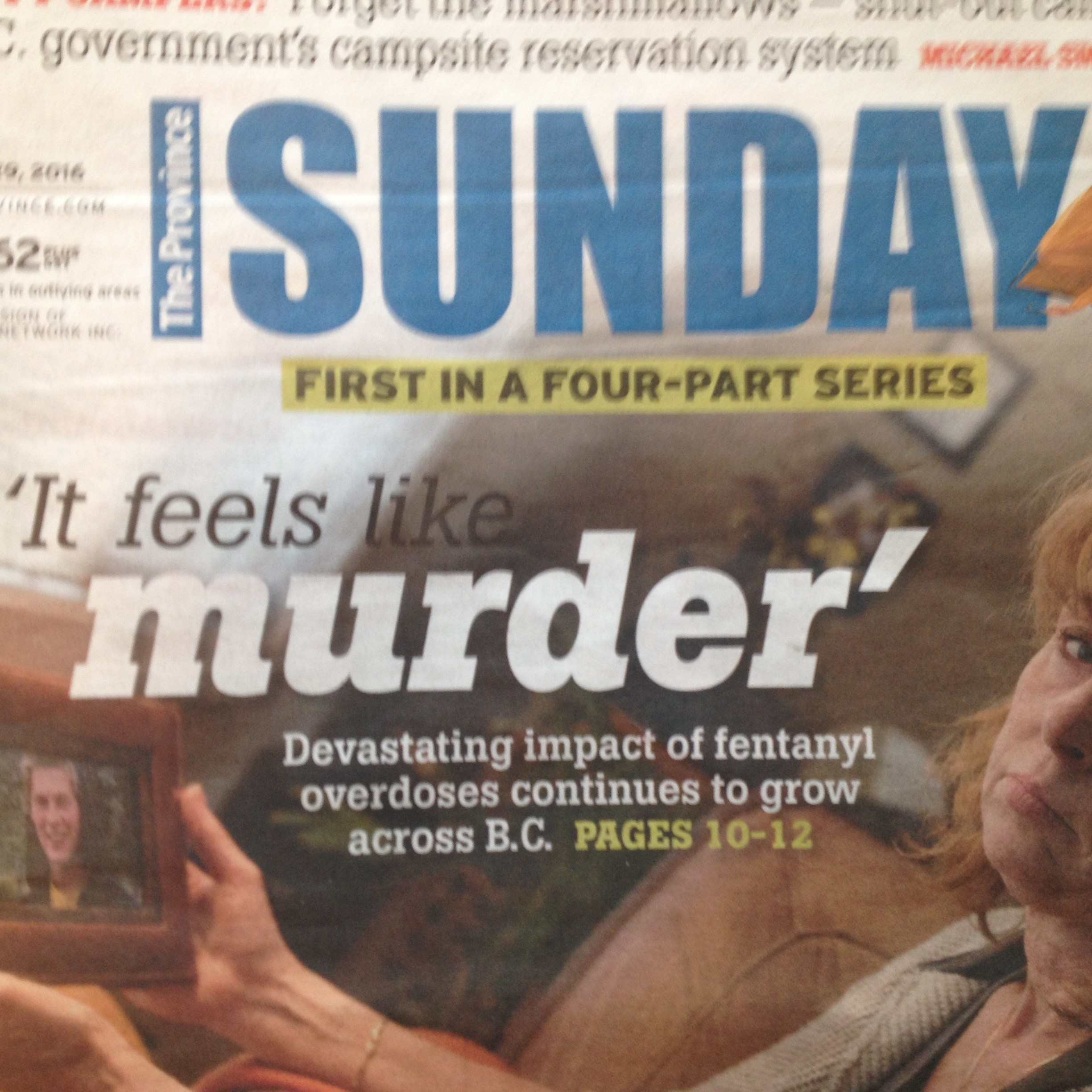
British Columbians, in Canada, are among the world’s most prolific illicit drug consumers and the B.C. Coroners Service just released some figures. They’re projecting over 800 drug overdose deaths for 2016. Maybe a thousand. Most will involve fentanyl.
Who is this lethal lady? Where does she come from? And why is she suddenly so popular?
 Fentanyl is a high-potency, rapid-onset synthetic opioid drug prescribed for the treatment of chronic pain. It was developed in the 1950’s as an intravenous anesthetic for surgery and evolved into a breakthrough cancer pain treatment in the form of tablets, lozenges, lollipops, and patches. It’s legal and readily available with a prescription and is listed on the U.S., Canadian, and U.K. Schedules as a controlled drug.
Fentanyl is a high-potency, rapid-onset synthetic opioid drug prescribed for the treatment of chronic pain. It was developed in the 1950’s as an intravenous anesthetic for surgery and evolved into a breakthrough cancer pain treatment in the form of tablets, lozenges, lollipops, and patches. It’s legal and readily available with a prescription and is listed on the U.S., Canadian, and U.K. Schedules as a controlled drug.
Like heroin and morphine, fentanyl works by binding to the body’s opiate receptors and driving up dopamine levels in the brain’s reward areas, producing a state of euphoria and intense relaxation. That’s all and well when used in moderation and highly effective when properly prescribed.
 But fentanyl is 100 times more potent than morphine and 50 times stronger than pharmaceutical grade, 100% pure heroin. It’s also far more available on the street than heroin and the reason is profit. One kilogram of heroin sells in Vancouver for $60,000—if you could find one. One kilo of fentanyl powder goes for $125,000 and is readily available. Not hard to figure out what’s going on.
But fentanyl is 100 times more potent than morphine and 50 times stronger than pharmaceutical grade, 100% pure heroin. It’s also far more available on the street than heroin and the reason is profit. One kilogram of heroin sells in Vancouver for $60,000—if you could find one. One kilo of fentanyl powder goes for $125,000 and is readily available. Not hard to figure out what’s going on.
But with fentanyl being so powerful, the inevitable deaths tag along. The mechanism of death by fentanyl overdose is the same as heroin in that the central nervous system is depressed and respiratory failure occurs. Fentanyl is much quicker than heroin, though. One street source was quoted, “With fentanyl you just hit the ground. Light’s out, that’s it. They don’t know there’s fentanyl in their fix till it’s too late.”
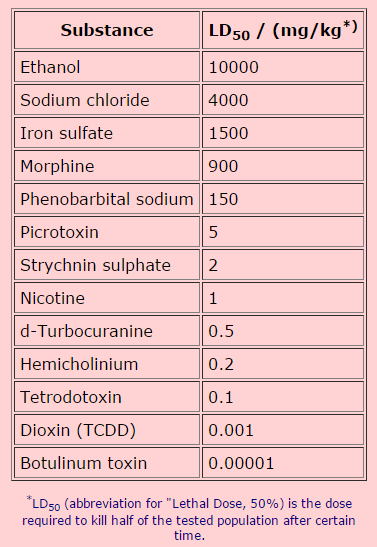
 The toxicity of all drugs is rated on an LD50 scale, whereas the Lethal Dose of 50 percent of humans occurs at a certain scale which is proportionate to body mass. Fentanyl’s LD50 rating is .03 mcg/kg (micrograms per kilogram). Given that a microgram is .001 of a milligram, this equals an average 70 kilogram (155 pound) person requiring 2.1 mgs of fentanyl to kill them. Some, already tolerant to opioids, require more. Some, with no tolerance, require less. Especially if mixed with other drugs or alcohol.
The toxicity of all drugs is rated on an LD50 scale, whereas the Lethal Dose of 50 percent of humans occurs at a certain scale which is proportionate to body mass. Fentanyl’s LD50 rating is .03 mcg/kg (micrograms per kilogram). Given that a microgram is .001 of a milligram, this equals an average 70 kilogram (155 pound) person requiring 2.1 mgs of fentanyl to kill them. Some, already tolerant to opioids, require more. Some, with no tolerance, require less. Especially if mixed with other drugs or alcohol.
So why the sudden rise in the availability of fentanyl?
There’ll always be the demand. The answer’s in the supply and the reason’s found on the internet. The digital drug highway. The internet has done to drugs what Amazon has done for books.
 Ten years ago, when heroin was so popular, it was available from a natural product through a complex delivery system which requires a chain from the country of source—China, Afghanistan, and Vietnam to name a few—through international couriers, middle-men, and street dealers before it ever reached the end-user. The junkie in the alley.
Ten years ago, when heroin was so popular, it was available from a natural product through a complex delivery system which requires a chain from the country of source—China, Afghanistan, and Vietnam to name a few—through international couriers, middle-men, and street dealers before it ever reached the end-user. The junkie in the alley.
The process of profit required “stepping-on” or “cutting” at every level and, by the time the drug reached the consumer, it was of low purity and the chances of an accidental overdose were slim.
Today’s plentiful purity is what’s killing the customers and it’s not about to change.
 Now you can go online and order any amount of fentanyl—a synthetic and easily mass-produced opioid—you want, as long as your money goes through. Visa, Mastercard, Paypal, and Bitcoin are fine and UPS will deliver it right to your door. Presto, you’re in the illicit drug business.
Now you can go online and order any amount of fentanyl—a synthetic and easily mass-produced opioid—you want, as long as your money goes through. Visa, Mastercard, Paypal, and Bitcoin are fine and UPS will deliver it right to your door. Presto, you’re in the illicit drug business.
Don’t believe me?
Well, I tried it out.
I started Google-searching “where to buy fentanyl online without a prescription” and snooped around. Then I hooked-up with a few shadowy and shady, sinister people through email. It’s easy to get information when you’re anonymous and they think you have money. They steered me to the Silk Road Online Pharmacy—the Walmart of internet black market pharmaceuticals. It’s in Karachi, Pakistan. Click here.

I paged through a menu of everything from Molly to Ecstacy to Pure MDMA to Phentermine to LSD to Viagara to Pregnyl to Humatrope. The site is nicely organized in departments with pretty much everything you could be surreptitiously looking for—men’s & women’s health, weight loss, pain-killers, things for ADD/ADHD, stuff for highs, shit for lows, a great selection of steroids, plus lots and lots of research chemicals and powders.
Then I found what I wanted.
Abstral.
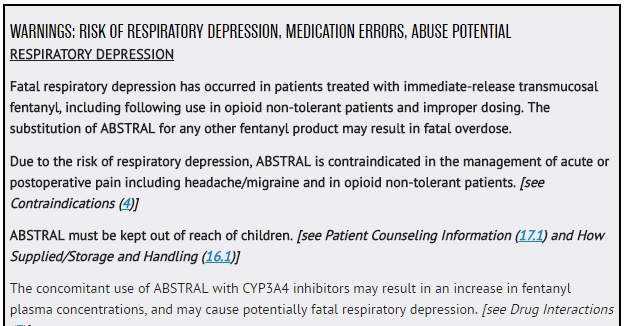
 Abstral is a brand name for a formulation of fentanyl citrate (the salt produced by combining the chemical base for fentanyl with citric acid) and is available as a sublingual tablet—one you dissolve under your tongue and is absorbed in your buccal mucosa to provide rapid analgesia. And it comes with this warning:
Abstral is a brand name for a formulation of fentanyl citrate (the salt produced by combining the chemical base for fentanyl with citric acid) and is available as a sublingual tablet—one you dissolve under your tongue and is absorbed in your buccal mucosa to provide rapid analgesia. And it comes with this warning:
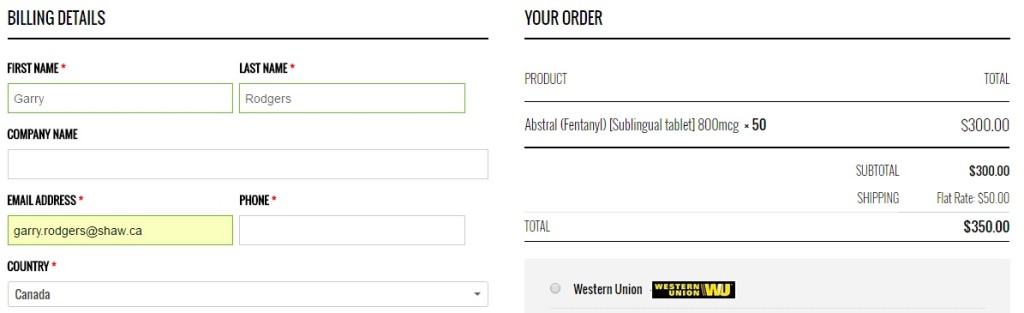
Silk Road Pharmacy sells Abstral in two strengths: 400 mcg and 800 mcg. I chose the stronger. There’s more bang for the buck.
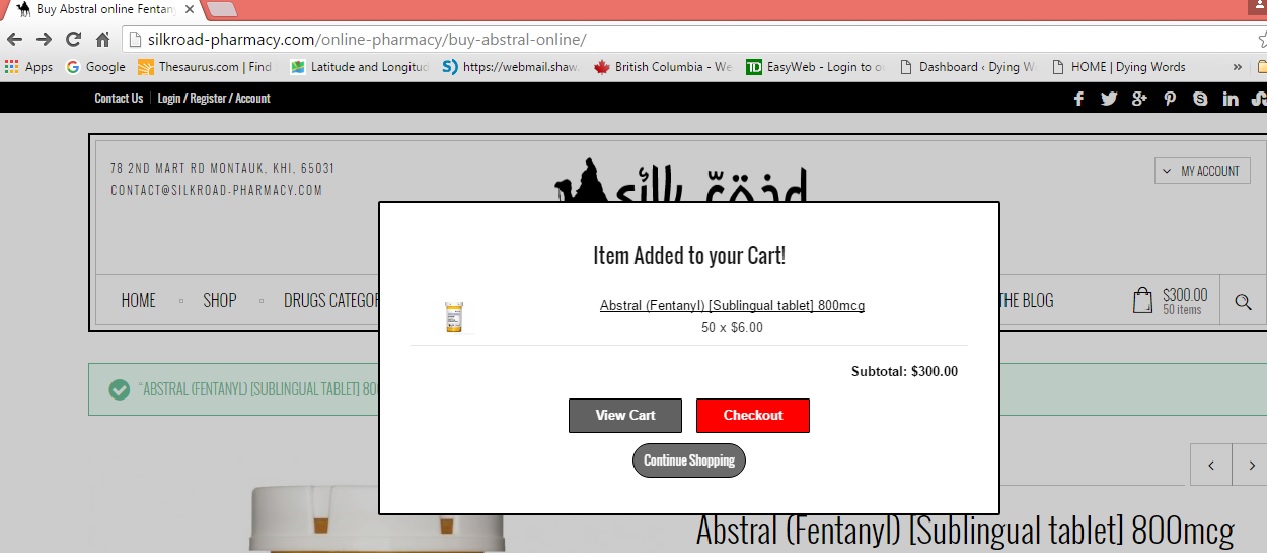
They also have a minimum order of 50 tablets so, being a first-time customer, I selected the lesser and clicked “Buy” on my cart. That took me to the checkout page where, for $300.00 plus fifty bucks for shipping and handling, the deal was done through my Mastercard. A client-needs agent by the name of Asha Ali guaranteed delivery to North America within two weeks. He even gave me his email at contact@silkroad.pharmacy.com if there’s a problem.
So, getting back to the not-so-hypothetical Fentanyl serial killer, this is what I’ve calculated. I have 50 – 800 microgram tabs of Abstral on the way. That’s a total of 40 milligrams. If it takes 2.1 mg to kill the average person, then I’ve got enough to do in nineteen people. Fifteen to be sure. Ten at the absolute least.
 Now, I don’t have anything against anyone in particular so I propose to do this randomly.
Now, I don’t have anything against anyone in particular so I propose to do this randomly.
What I’ve got in mind is cruising the coffee shops downtown. There’s Starbucks at the mall. The Vault on the corner. Serious Coffee in the conference center. Perkins up the street. And there’s got to be twenty restaurants with three blocks. It’ll be so easy to grind up my e-mail pills and sprinkle the fentanyl powder into momentarily unattended lattes. I might even lace sugar packets.
Hey! Imagine the bars where they’re drinking.
 Talk about a return on the dollar. That’s under twenty-five bucks a death—the price of five coffees at Starbucks—three beers and a burger at The Palace. The chances of getting caught are practically nil. Random stranger-to-stranger killings are the hardest to solve and the easiest to get away with. Just ask the Chicago Tylenol Poisoner.
Talk about a return on the dollar. That’s under twenty-five bucks a death—the price of five coffees at Starbucks—three beers and a burger at The Palace. The chances of getting caught are practically nil. Random stranger-to-stranger killings are the hardest to solve and the easiest to get away with. Just ask the Chicago Tylenol Poisoner.
Anyway, I have a couple weeks before my precious pills get here—a couple weeks plotting serial kills with fentanyl poisoning. It’s my next novel.
And I’m planning a plot with a random twist that you’ll never see coming… in Deadly Little Sister.