 The word “psychopath” conjures images of fictional psychos like Norman Bates, Hannibal Lecter, and Annie Wilkes, as well as reality monsters such as Ted Bundy, John Wayne Gacy, and Eileen Wuornos. However, proven clinical studies show 3% of the world’s population have psychopathic psychological profiles—most being men. Surprisingly, few are actually violent. But they’re out there… all around you… and they’re hiding in plain sight.
The word “psychopath” conjures images of fictional psychos like Norman Bates, Hannibal Lecter, and Annie Wilkes, as well as reality monsters such as Ted Bundy, John Wayne Gacy, and Eileen Wuornos. However, proven clinical studies show 3% of the world’s population have psychopathic psychological profiles—most being men. Surprisingly, few are actually violent. But they’re out there… all around you… and they’re hiding in plain sight.
Psychopaths aren’t specifically defined under the American Psychiatric Association’s Diagnostic and Statistical Manual Five, (DSM-5) which is the profession’s bible when it comes to profiling abnormal behavior. Psychopathy and it’s alter-ego, sociopathy, are jointly classified as Antisocial Personality Disorders and are diagnosed according to specific behaviors.
 Part of identifying a psychopathic character is applying the 40 Point Revised Psychopathy Checklist (PCL-R) which is a categorical diagnosis developed by psychologist, Dr. Robert Hare, who studied prison inmates. It indicates a psychopathic personality through a psychometric dimensional score. It’s a recognized process for legal, clinical, and research purposes. Interestingly, a version of the Psychopathy Checklist is available online and I’ve linked it for you. Take it. I’m curious if you’re more psychopathic than me. I tried the test—and I’ll show you my score—if you stick reading this article.
Part of identifying a psychopathic character is applying the 40 Point Revised Psychopathy Checklist (PCL-R) which is a categorical diagnosis developed by psychologist, Dr. Robert Hare, who studied prison inmates. It indicates a psychopathic personality through a psychometric dimensional score. It’s a recognized process for legal, clinical, and research purposes. Interestingly, a version of the Psychopathy Checklist is available online and I’ve linked it for you. Take it. I’m curious if you’re more psychopathic than me. I tried the test—and I’ll show you my score—if you stick reading this article.
But before you go ahead and answer the forty question, true-or-false test, let’s look at the parameters of abhorrent behavior and how it applies to whether or not you’re psychopathic.
The DSM-5 recognizes six general personality disorders:
- Borderline
- Avoidant
- Narcissistic
- Obsessive-Compulsive
- Antisocial
- Schizotypal
Quoting directly from the DSM-5:
 The essential features of a personality disorder are impairments in personality (self and interpersonal) functioning and the presence of pathological personality traits. To diagnose antisocial personality disorder, the following criteria must be met:
The essential features of a personality disorder are impairments in personality (self and interpersonal) functioning and the presence of pathological personality traits. To diagnose antisocial personality disorder, the following criteria must be met:
Significant impairments in personality functioning manifest by:
1. Impairments in self-functioning (a or b):
(a) Identity: Ego-centrism; self-esteem derived from personal gain, power, or pleasure.
(b) Self-direction: Goal-setting based on personal gratification; absence of prosocial internal standards associated with failure to conform to lawful or culturally normative ethical behavior.
AND…
2. Impairments in interpersonal functioning (a or b):
(a) Empathy: Lack of concern for feelings, needs, or suffering of others; lack of remorse after hurting or mistreating another.
(b) Intimacy: Incapacity for mutually intimate relationships, as exploitation is a primary means of relating to others, including by deceit and coercion; use of dominance or intimidation to control others.
Pathological personality traits in the following domains:
 1. Antagonism, characterized by:
1. Antagonism, characterized by:
(a) Manipulativeness: Frequent use of subterfuge to influence or control others; use of seduction, charm, glibness, or ingratiation to achieve one’s ends.
(b) Deceitfulness: Dishonesty and fraudulence; misrepresentation of self; embellishment or fabrication when relating events.
(c) Callousness: Lack of concern for feelings or problems of others; lack of guilt or remorse about the negative or harmful effects of one’s actions on others; aggression; sadism.
(d) Hostility: Persistent or frequent angry feelings; anger or irritability in response to minor slights and insults; mean, nasty, or vengeful behavior.
2. Disinhibition, characterized by:
 (a) Irresponsibility: Disregard for – and failure to honor – financial and other obligations or commitments; lack of respect for – and lack of follow through on – agreements and promises.
(a) Irresponsibility: Disregard for – and failure to honor – financial and other obligations or commitments; lack of respect for – and lack of follow through on – agreements and promises.
(b) Impulsivity: Acting on the spur of the moment in response to immediate stimuli; acting on a momentary basis without a plan or consideration of outcomes; difficulty establishing and following plans.
(c) Risk taking: Engagement in dangerous, risky, and potentially self-damaging activities, unnecessarily and without regard for consequences; boredom proneness and thoughtless initiation of activities to counter boredom; lack of concern for one’s limitations and denial of the reality of personal danger.
Overall factors to consider:
 The impairments in personality functioning and the individual‟s personality trait expression are relatively stable across time and consistent across situations.
The impairments in personality functioning and the individual‟s personality trait expression are relatively stable across time and consistent across situations.- The impairments in personality functioning and the individual‟s personality trait expression are not better understood as normative for the individual‟s developmental stage or sociocultural environment.
- The impairments in personality functioning and the individual‟s personality trait expression are not solely due to the direct physiological effects of a substance (e.g., a drug of abuse, medication) or a general medical condition (e.g., severe head trauma).
- The individual is at least age 18 years and shows an established history of juvenile conduct disorder.
So the DSM-5 clearly lays out what constitutes Antisocial Behavior Disorder. But we’re used to hearing the terms “Psychopath” and “Sociopath”. Is there a difference?
Non-clinically, yes. The best description seems to be that psychopaths are born and sociopaths are made. It’s a nature versus nurture debate. Innate versus learned behaviors.
Psychopaths and sociopaths are both social predators and share the same characteristics of lack or empathy, remorse, or guilt. They don’t take responsibility for their own actions. They disregard social norms and conventions. Laws are for others. They incline towards violence. And, to their core, they’re manipulative and deceitful.
 Sociopaths generally come from the lower elements in life—poor socio-economic families, poor education, poor health with addiction issues—and they’re highly impulsive, not inclined to plan-out events nor to exhibit much patience. Sociopaths are usually loners with miserable attitudes and are ostracized by society—mostly unemployable. Their emotional level is primitive and they have little fear with the exception of personal injury and dying. Sociopaths can be thought as rudimentary or undeveloped psychopaths that want little to do with society.
Sociopaths generally come from the lower elements in life—poor socio-economic families, poor education, poor health with addiction issues—and they’re highly impulsive, not inclined to plan-out events nor to exhibit much patience. Sociopaths are usually loners with miserable attitudes and are ostracized by society—mostly unemployable. Their emotional level is primitive and they have little fear with the exception of personal injury and dying. Sociopaths can be thought as rudimentary or undeveloped psychopaths that want little to do with society.
Psychopaths, on the other hand, are much more intelligent and mix well in society. They’re  usually educated and employed—some holding high degrees, responsible positions, and even elected office. They are generally much healthier than sociopaths and not as prone to substance abuse. Psychopaths are cunning. They’ll plan to the tiniest detail when committing crimes or deceiving others. They’re completely aware of what they’re doing and it’ll always be in their interest, with a focus on minimizing risk to themselves. Psychopaths are slightly more emotional than sociopaths, however these emotions are the destructive ones of hate, disgust, contempt, and revenge.
usually educated and employed—some holding high degrees, responsible positions, and even elected office. They are generally much healthier than sociopaths and not as prone to substance abuse. Psychopaths are cunning. They’ll plan to the tiniest detail when committing crimes or deceiving others. They’re completely aware of what they’re doing and it’ll always be in their interest, with a focus on minimizing risk to themselves. Psychopaths are slightly more emotional than sociopaths, however these emotions are the destructive ones of hate, disgust, contempt, and revenge.
It’s said that in the game of life, psychopaths know what cards you’re holding, and they cheat.
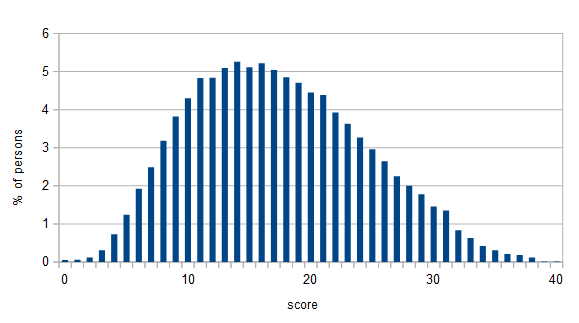 So, are you ready to see where your personality fits on the bell-curve chart of psychopathy? Here are the 40 standard questions on the PCL-R that must be answered either true or false as it applies to you. There’re no “in-betweens”, “kindas”, or “sort-ofs”. It’s black or white. To have your psychopathic traits scored, go to the online site at http://vistriai.com/psychopathtest/. Click Here
So, are you ready to see where your personality fits on the bell-curve chart of psychopathy? Here are the 40 standard questions on the PCL-R that must be answered either true or false as it applies to you. There’re no “in-betweens”, “kindas”, or “sort-ofs”. It’s black or white. To have your psychopathic traits scored, go to the online site at http://vistriai.com/psychopathtest/. Click Here
The Psychopath Test
What is your age?
What gender do you identify as?
__ Man.
__ Woman.
Mark each of the items below as true or false when applied to you.
1. I never, never get tongue-tied.
__ True __ False
2. In important ways, I am superior to most people.
__ True __False
3. I am prone to boredom.
__ True __False
4. I lie to make things go smoother.
__True __False
5. I cheat people out of things.
__True __False
6. I rarely feel guilty.
__True __False
7. I am an emotional person.
__True __False
8. I rarely connect emotionally with others.
True. False.
9. I often get others to pay for things for me.
__True __False
10. I am impatient.
__True False
11. I am promiscuous.
__True __False
12. I was a problem child.
__True __False
13. I have difficulty staying committed to long term goals.
__True __False
14. I am impulsive.
__True __False
15. I frequently perform sloppy work.
__True __False
16. I try to evade responsibility.
__True __False
17. My romantic relationships usually fall apart quickly.
__True __False
18. I committed some crimes as a juvenile.
__True __False
19. I have violated a probation order.
__True __False
20. I have committed many types of crimes.
__True __False
21. I am neither shy nor self-conscious; I speak with authority.
__True __False
22. I am exceptional.
__True __False
23. I need to take risks to feel alive.
__True __False
24. I am basically an honest person.
__True __False
25. I feel bad when I trick people.
__True __False
26. If someone deserves it, I don’t feel too bad.
__True __False
27. I think strong emotions are for the weak.
__True __False
28. I think if people get offended, that is their problem.
__True __False
29. I have always taken care of myself.
__True __False
30. I never act hastily.
__True __False
31. I think sex should not be taken lightly.
__True __False
32. I was often in trouble at school.
__True __False
33. I lack direction in my life.
__True __False
34. I never give in to temptation.
__True __False.
35. I always keep my word.
__True. __False
36. My problems are mostly the fault of others.
__True __False
37. I don’t like to commit in relationships.
__True __False
38. I was a bully in high school.
__True __False
39. I have been held in contempt of court.
__True __False
40. I am not or would not be proud of getting away with crimes.
__True __False
Again, to take the test online and have it scored, go to http://vistriai.com/psychopathtest/. Click Here
Don’t be worried unless you scored 25. That’s the threshold for psychopathy. Anything over 30—you should be seriously concerned. And above 35, you’re in the company of greats. Eileen Wuronos scored 35. John Wayne Gacy was 36. Canadian superstars Paul Bernardo and Clifford Olson were 37 and 38, respectively. Little known USA serial killer Peter Lundin got a 39. And Theodore Bundy aced it. 40 outa 40.